Causes2,3
- Cerebral palsy (CP)
- Traumatic brain injury or spinal cord injury
- Stroke (ischemic or hemorrhagic)
- Brain damage caused by oxygen deficiency
- Multiple sclerosis
- Encephalitis or meningitis
- Brain tumor sequelae

Symptoms4
- Muscle stiffness (known as hypertonia)
- Limited range of movement
- Reduced ability to relax muscles
- Muscle spasms
- Changes in limb position
- Pain
Common Occurrence after TBI5
- Spasticity may be one of the many possible consequences after a traumatic brain injury (TBI)
- An estimated 475,000 children between 0-14 years of age sustain a TBI annually
- In pediatric spasticity, MRI imaging shows damage to or development differences in the motor cortex
Clinical Patterns4





Elijah Is a 9-year-old Soccer Player Who STAYS POSITIVE On and Off the Field
The life he's fighting for
From the time he was young, Elijah has loved being a leader. He inspires his soccer teammates with confidence and optimism—scoring goals and starting cheers. When his younger siblings or parents need help, he always leads the charge.

The weigh-in
- When Elijah was 6 years old, he developed upper limb spasticity following a traumatic brain injury
- Sometimes he experiences difficulty writing, changing clothes, and playing with friends
- Socially, symptoms of upper limb spasticity can often get in the way and make it more difficult to connect with classmates or teammates
Sparring with upper limb spasticity
- For a few years after the accident, Elijah adjusted his life to live with the symptoms of upper limb spasticity, receiving physical therapy
Never defeated, Elijah and his mom looked at options
The Pediatric Portfolio
Watch a pediatric physiatrist discuss the safety and efficacy of XEOMIN for approved pediatric indications
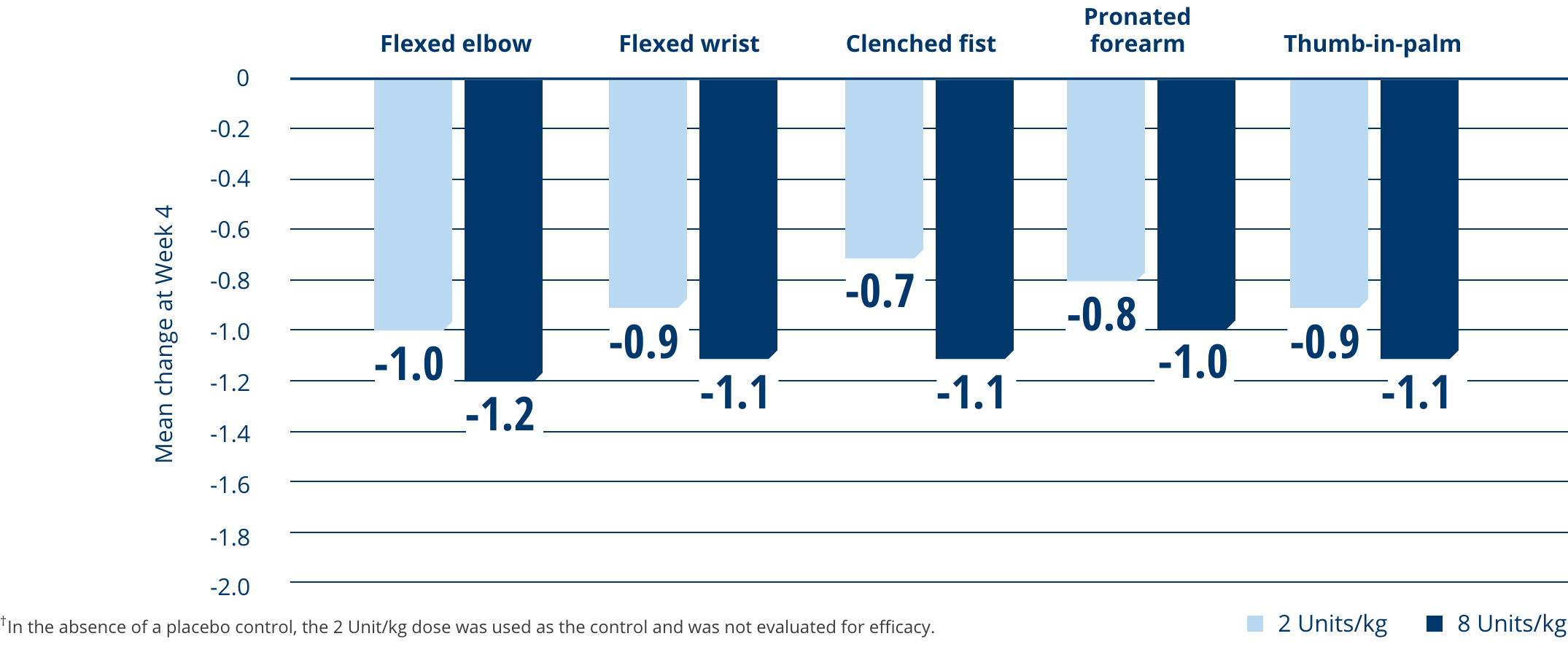
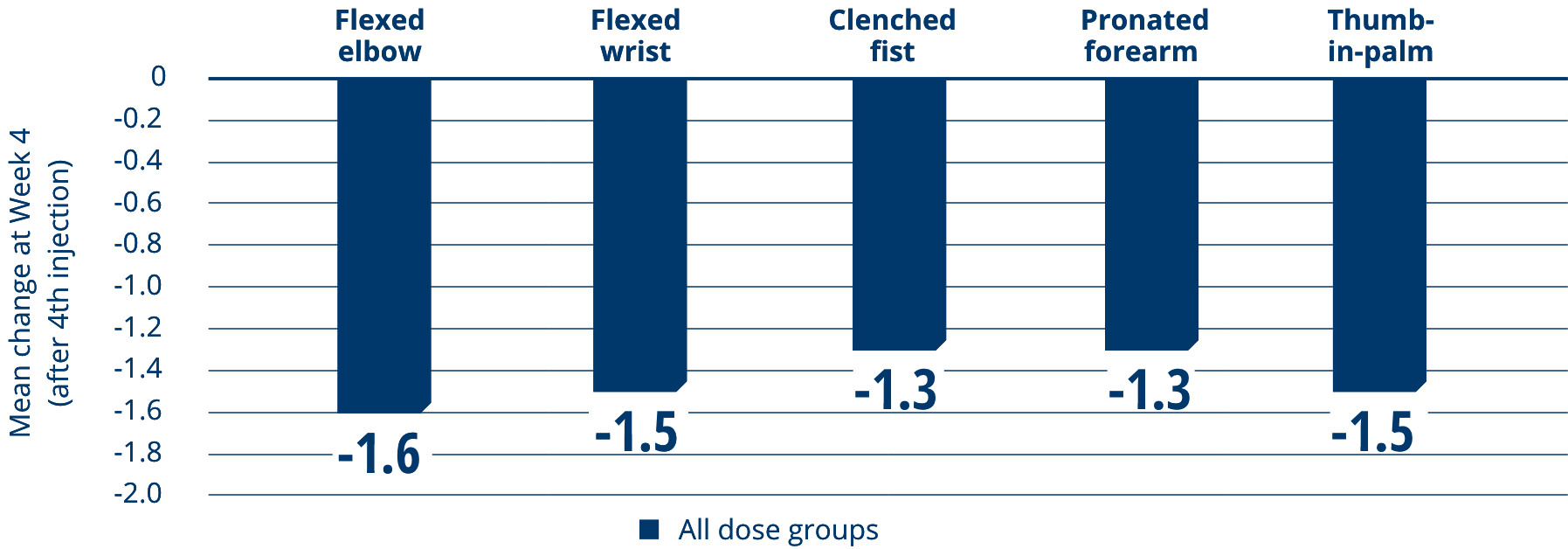
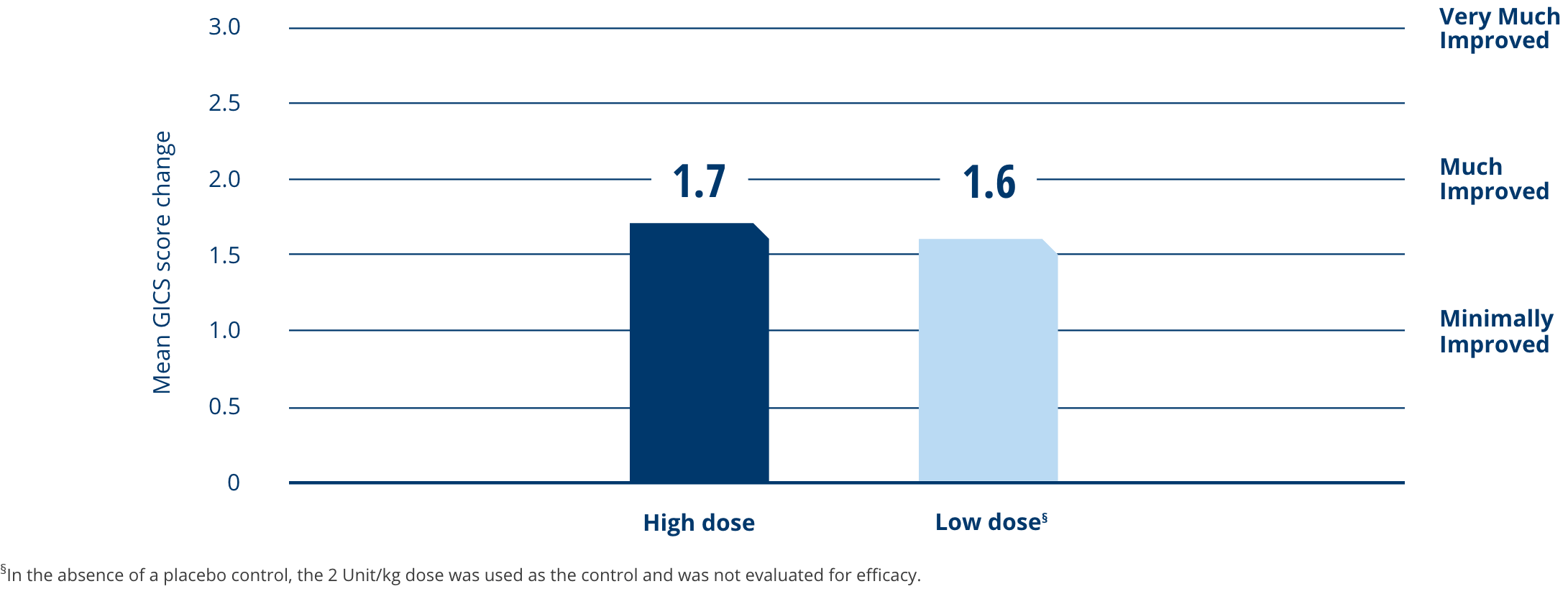
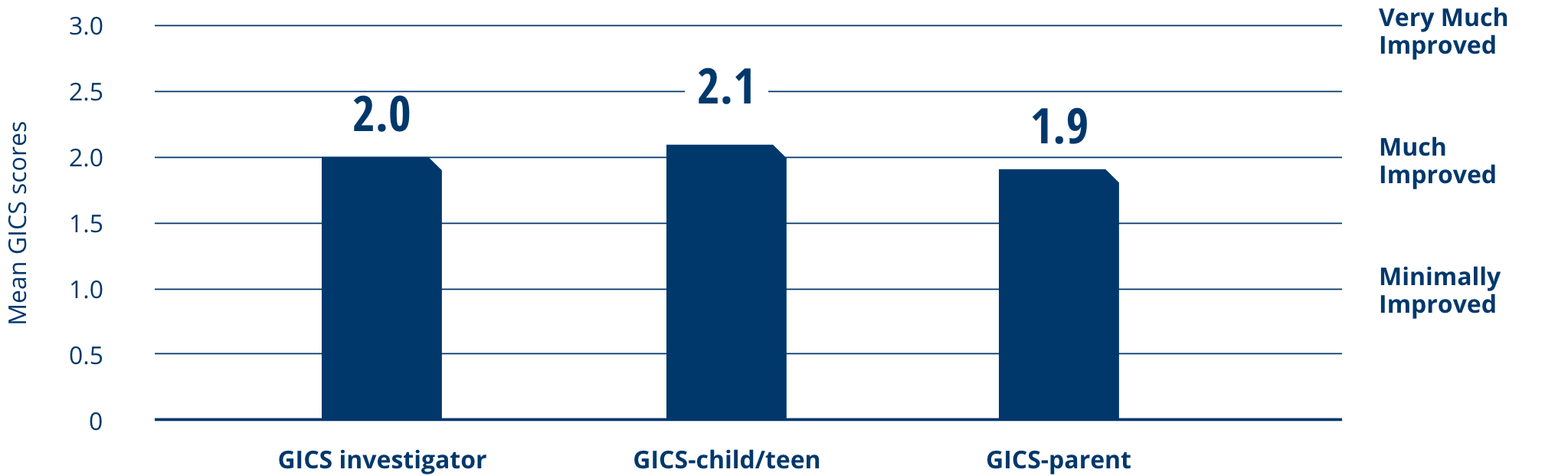
Explore XEOMIN for the treatment of pediatric upper limb spasticity†
See the XEOMIN Difference
XEOMIN® (incobotulinumtoxinA) for injection is indicated for the treatment of upper limb spasticity in pediatric patients 2 to 17 years of age, excluding spasticity caused by cerebral palsy. A pediatric assessment for XEOMIN demonstrates that XEOMIN is safe and effective in cerebral palsy patients. XEOMIN is not approved for this specific patient population due to marketing exclusivity for another botulinum toxin.
TBI, traumatic brain injury.